








































 प्रतीकात्मक चित्र
प्रतीकात्मक चित्र
Objective: To determine the efficacy and safety of awake prone positioning versus usual care in non-intubated adults with hypoxemic respiratory failure due to covid-19.
Design: Systematic review with frequentist and bayesian meta-analyses.
Study eligibility: Randomized trials comparing awake prone positioning versus usual care in adults with covid-19 related hypoxemic respiratory failure. Information sources were Medline, Embase, and the Cochrane Central Register of Controlled Trials from inception to 4 March 2022.
Data extraction and synthesis: Two reviewers independently extracted data and assessed risk of bias. Random effects meta-analyses were performed for the primary and secondary outcomes. Bayesian meta-analyses were performed for endotracheal intubation and mortality outcomes. GRADE certainty of evidence was assessed for outcomes.
Main outcome measures: The primary outcome was endotracheal intubation. Secondary outcomes were mortality, ventilator-free days, intensive care unit (ICU) and hospital length of stay, escalation of oxygen modality, change in oxygenation and respiratory rate, and adverse events.
Results: 17 trials (2931 patients) met the eligibility criteria. 12 trials were at low risk of bias, three had some concerns, and two were at high risk. Awake prone positioning reduced the risk of endotracheal intubation compared with usual care (crude average 24.2% v 29.8%, relative risk 0.83, 95% confidence interval 0.73 to 0.94; high certainty). This translates to 55 fewer intubations per 1000 patients (95% confidence interval 87 to 19 fewer intubations).
Awake prone positioning did not significantly affect secondary outcomes, including mortality (15.6% v 17.2%, relative risk 0.90, 0.76 to 1.07; high certainty), ventilator-free days (mean difference 0.97 days, 95% confidence interval −0.5 to 3.4; low certainty), ICU length of stay (−2.1 days, −4.5 to 0.4; low certainty), hospital length of stay (−0.09 days, −0.69 to 0.51; moderate certainty), and escalation of oxygen modality (21.4% v 23.0%, relative risk 1.04, 0.74 to 1.44; low certainty).
Adverse events related to awake prone positioning were uncommon. Bayesian meta-analysis showed a high probability of benefit with awake prone positioning for endotracheal intubation (non-informative prior, mean relative risk 0.83, 95% credible interval 0.70 to 0.97; posterior probability for relative risk <0.95=96%) but lower probability for mortality (0.90, 0.73 to 1.13; <0.95=68%).
Conclusions: Awake prone positioning compared with usual care reduces the risk of endotracheal intubation in adults with hypoxemic respiratory failure due to covid-19 but probably has little to no effect on mortality or other outcomes.







नेचर कम्युनिकेशंस जर्नल में प्रकाशित नई स्टडी बताती है कि वे अब अंग्रेजी वर्णमाला के 26 अक्षरों को

मेडिकल कॉलेज चिकित्सालय के नेत्र रोग विभाग में जल्द ही नेत्र बैंक स्थापित होगा। यहां कार्निया ट्रांस
उपमुख्यमंत्री बृजेश पाठक ने योगी सरकार -2 के 100 दिन पूरे होने पर लोक भवन में स्वास्थ्य विभाग की रिप

प्रधानमंत्री नरेन्द्र मोदी (Narendra Modi) ने अधिक से अधिक लोगों को 21 जून को अंतरराष्ट्रीय योग दिवस

'हर घर दस्तक' मुहिम के तहत स्वास्थ्यकर्मी घर-घर जाकर लोगों को टीका लगाएंगे। इस दौरान दूसरे डोज से वं

कैलिफ़ोर्निया के बादाम एक प्राकृतिक, संपूर्ण और उच्च गुणवत्ता वाला आहार हैं। अल्मंड बोर्ड ऑफ कैलिफ़ो

मौसम बदलने के साथ ही गले में खराश होना एक आम समस्या बन जाती है लेकिन कुछ ऐसे घरेलू तरीकों से गले की

कल के इस सम्मान समारोह में कास मेहमानों में अपर पुलिस महानिदेशक गोरखपुर जोन अखिल कुमार, पुलिस उपमहा

प्रदेश के 107 जिला अस्पताल सीसी कैमरों से लैस हो गए हैं। इन कैमरों के जरिए 24 घंटे अस्पतालों पर नजर

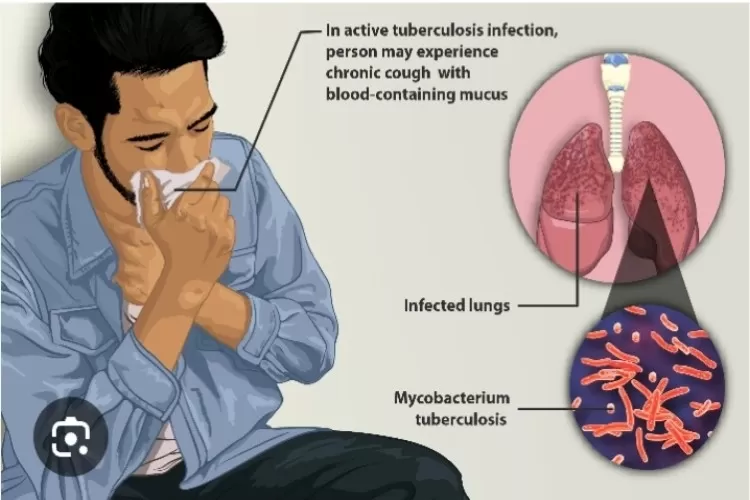
डब्ल्यूएचओ सभी को टीबी से पीड़ित लोगों के प्रति सहानुभूति व मदद का भाव रखने के साथ ही, बीमारी को समझ


















{kind=link}
COMMENTS